

TAP
 Though the TAP block tends to be one that people venture into after they have started with at least a few of the orthopedic blocks, I would recommend putting it on the short list of blocks to learn even if you are just starting to use ultrasound. It is a very easy block to learn and perform, especially for single injections because it is relatively superficial, and there are few items to interpret on ultrasound. Further, it is a very ‘forgiving’ block, and there are a variety of opportunities to utilize this block in your practice. There are some advanced skills to master to achieve superior analgesia and extend block length (and I will discuss some of these in future updates), but achieving great analgesia with this block can be accomplished with easily even early in your skills development. Speaking of easy, the SUBCOSTAL TAP technique is even easier to perform!
Though the TAP block tends to be one that people venture into after they have started with at least a few of the orthopedic blocks, I would recommend putting it on the short list of blocks to learn even if you are just starting to use ultrasound. It is a very easy block to learn and perform, especially for single injections because it is relatively superficial, and there are few items to interpret on ultrasound. Further, it is a very ‘forgiving’ block, and there are a variety of opportunities to utilize this block in your practice. There are some advanced skills to master to achieve superior analgesia and extend block length (and I will discuss some of these in future updates), but achieving great analgesia with this block can be accomplished with easily even early in your skills development. Speaking of easy, the SUBCOSTAL TAP technique is even easier to perform!
Whether we are targeting the inguinal area or the lower abdomen, we still usually just call this a TAP block instead of saying that we are doing an ILIOINGUINAL/ILIOHYPOGASTRIC (II/IH) BLOCK. There is a CPT code for ‘Other’ that can be used for a TAP block and a CPT code for II/IH block that can be used depending on how you view this nuance.
The cadaver picture below will shed some light on this concept. The Right of the picture is Cranial, and the Lower aspect is Lateral. The muscle fibers oriented vertically at the top of the picture are the TRANSVERSUS ABDOMINUS muscles with the top extending toward the midline. The ANTERIOR BRANCHES OF THE SUBCOSTAL NERVES can be seen segmentally running just above the transversus muscle. The more superficial layers of the abdomen have been peeled away toward the mid-axillary line and lie at the bottom of the photo. The fascial layer seen peeled back is the target of our TAP block. A LATERAL BRANCH OF A SUBCOSTAL NERVE can be seen diving under (going superficial to) this fascial plane into the internal oblique muscle. Note as well, there are blood vessels to remain aware of during this nerve block.

The next cadaver picture highlights the II/IH nerves under the fascial plane running from the center of the picture toward the lower left of the photo. At this point, they have pierced the fascial layer, also going superficially in a medial and caudad direction. If you imagine the peeled back tissue folded back into place, it is more clear that these nerves are headed in the correct direction. Note also in this photo the right border of the peeled back tissue layers demonstrates the fascial layer between the internal and external oblique muscles as well as the torn edges of the external obliques muscles.

Our surgical site can influence where we prefer to deposit our local anesthetic for optimal benefit. Remember that I mentioned that this block is ‘forgiving’, so I would not try too long to be perfect (wasting valuable time or worse, inadvertently entering the bowel), but do take the time necessary to confirm that you are not depositing the local within the body of either the internal oblique or transverse abdominus muscle.
The advantage of perineural versus infiltrative (field) blocks is the deposition of local anesthetic in a relatively inaccessable (to the vasculature) plane, diminishing the plasma levels and extending the duration of the local anesthetic. Placing the local within the TAP fascia does this best. Placing the local just above or below the fascia will provide adequate analgesia even if the local has to cross to the other side of the fascia reach the target nerves. Digging in the more lateral edge of the probe allows for a more flat angle of approach to the ultrasound probe. Even infusion rates can be run at relatively low rates which is good because four catheters might be used for an exploratory laparotomy (though there are other strategies for handling this situation!).
If our target is a midline lower abdominal incision, then we[nonmember]…
REGISTER for FREE to become a SUBSCRIBER or login HERE to view the full article!
[/nonmember]
[ismember]
[wlm_ismember]
only need to block the anterior branches which remain under the TAP fascia. It is fine to just go lateral enough to see the ‘layers of cake’ and inject below the TAP fascia, peeling the transversus abdominus muscle down off of the fascia. This will result in the fastest onset in my experience. It is unnecessary to locate or block the II/IH nerves.
If we are doing a colostomy, then it becomes necessary to follow the muscular planes as far back as the mid-axillary line to make sure the lateral branches which innervate the lateral aspect of the abdomen are covered. Remember, we saw the lateral branch exiting superficially in the first cadaver photo. Sometimes going more lateral results in a degraded image, and the orientation to the screen gets turned 90 degrees.
If our surgery is for an inguinal hernia or endovascular aortobifemoral repair (yes, I have done continuous bilateral TAP blocks for this; awesome story for another posting!), then our target nerves include the II/IH nerves which can often be recognized in or above the the TAP fascia in a more anterior location as an elongated white thickening in the fascial plane , often containing hypoechoic circles. If they are not easily seen, I go back as far as I have a good view and aim at injecting within the TAP fascia. This creates a line above and below the local from the single white line seen on ultrasound. I have found this much easier to accomplish using a sharp needle than with a Tuohy needle. You often find yourself scraping along the fascia a while with the latter. If this ‘double line’ cannot be achieved farther around toward the axilla(which will allow our local to remain in place for an extended period of time), then the very close second best option is to to the following. Follow the three layers just far enough for a good view and inject above the TAP fascial layer (but below the Internal Oblique muscle). Remember that we saw the II/IH nerves emerge through this fascial plane in a superficial course heading medially for an extended length just superficial to the TAP fascia. We can catch them medially just outside this plane. Again, you may even see the bundle on ultrasound.
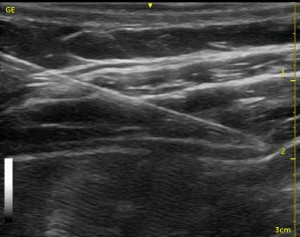
The below ultrasound image can not demonstrate the relative ease of determining the exact location of each of the muscular layers because you do not see the bowels moving and do not get to orient yourself by starting at the rectus muscle. In this image, the thickest layer is the internal oblique muscle, and the dark area just below that is the transversus abdominus muscle. The white line between these muscles is the fascia representing the TAP. Below the transversus abdominus muscle is a wide shimmering white area which represents the bowels. The II/IH nerves are seen as a white thickened area in the TAP fascia at about the middle of the image.

Watch the video below to see a TAP scan starting at the rectus muscle:
Watch the following video to see Great TAP Spread:
[/wlm_ismember]
See Also: Analgesia for Ex Lap, Back On Their Feet Again, Ultrasound Tip #3, TAP Block Pain Evaluation, Evaluating your TAP Block Injection