

SUPRACLAVICULAR
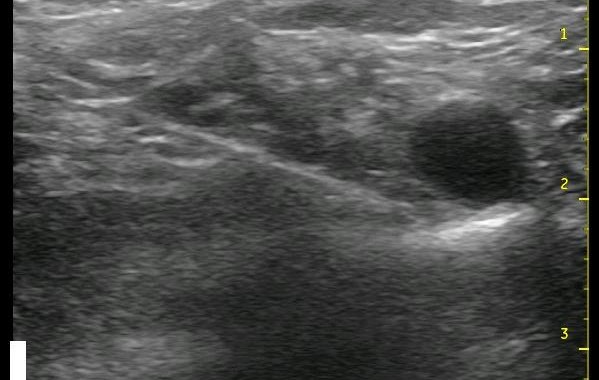
Above, you can see a needle advancing from the left of the image and piercing the middle scalene muscle to approach the ‘corner pocket’ at 2 cm depth. The muscle is indistinct due to the very steep angle at which it is being viewed. The ‘corner pocket’ is at the intersection of the rib, artery.. read more →
SUBGLUTEAL SCIATIC
The subgluteal approach is where I first started blocking the sciatic nerve for total knee arthroplasty (TKA). Since I usually performed the subgluteal sciatic nerve block as a single injection (and some of the extra steps for a continuous block could be omitted) after the continuous femoral block was already secured in place,.. read more →
SAPHENOUS
This is an often overlooked nerve block for ankle and foot procedures. This furthest extension of the femoral nerve has no motor component. It serves sensory innervation to the medial aspect of the calf including the ankle and some degree of the medial aspect of the forefoot. It also has a small contribution.. read more →
POPLITEAL SCIATIC
I consider this block to be one of the basic blocks that should be learned early in the course of converting to ultrasound and continuous nerve blocks. Of the sciatic nerve blocks, it is the easiest to incorporate ultrasound (no matter your original approach or patient positioning), it is a superficial block which.. read more →
PARAVERTEBRAL
This is not a block that you should cut your teeth on, but it is the one that, in my opinion, has the most dramatic impact on the recovery of my patients. It is just awesome to speak to a patient after a thoracotomy that can take a deep breath and cough easily.. read more →
LUMBAR PLEXUS
I find this block to be one of the few, whether single injection or continuous, where the impact of ultrasound utilization is not as dramatic an improvement as it is with most other nerve blocks. This comes from a few different variables. One, it is usually a deep block, so visualization of structures.. read more →
FEMORAL

The femoral nerve is seen to the left of the femoral artery and vein as a hyperechoic (white) triangle in the ultrasound image to the left. This is often one of the first nerve block to master with ultrasound because it is a relatively simple and superficial option and also probably because Total.. read more →
FASCIA ILIACA
I know I keep saying that this or that block is one of the ‘easy ones’, but this one really is another one of them. There are only a few simple essentials to identify on the image, and this block is also a good one to perform early as you are developing ultrasound.. read more →
INTERSCALENE

Converting from nerve stimulation to ultrasound for an interscalene nerve block classically involves going to a more posterior approach. This is also the case when changing from the traditional single injection to a continuous nerve block. For reasonable catheter securement issues as well as optimizing visualization with ultrasound, it becomes necessary to enter the skin several.. read more →
SUBCOSTAL TAP
As I mentioned in the previous section, I believe that the subcostal TAP block is even easier than the TAP block. With the TAP block, the main difficulty is getting within (or just below or above) the fascial plane without puncturing the bowel. This can involve a significant amount of scraping or jabbing.. read more →